
Introduction to Weight Management and Obesity
As most of you know, weight management and obesity are growing problems worldwide: more and more people suffer daily!
We’ll start by looking at ways to assess obesity. You’ve probably heard of the term: BMI or Body Mass Index, but there are other ways to evaluate obesity. And assess fat distribution, where the fat is stored in the body, is an important measurement.
One of the reasons healthcare experts are concerned about obesity is that it’s associated with health risks, other diseases, and an increased risk for diabetes.
We’ll know the term: “Metabolic Syndrome” – a critical topic we need to address is why people develop obesity. We’ll look at it from different angles: the psychological and social grade, the environment’s role, and the changing climate nowadays, with lots of food. Moreover, we’ll look at the genetics part because this turns out to be quite substantial, at least in some people.

Now a key question to all of this is: What can we do about this? So no worries! As we go through the changes in the so-called obesogenic environment, we’ll know about the changes that promote obesity, the abundance of food, and the little exercise we need to do to get to our grocery store or work. All of this needs to be changed, and we must address how we can accomplish that.
So this will be a lot of fun, and I’m happy you’re reading it.
Enjoy!
Assessing Obesity

Let’s Get to Know the Most Common Term Related to Obesity
Body Mass Index (BMI)
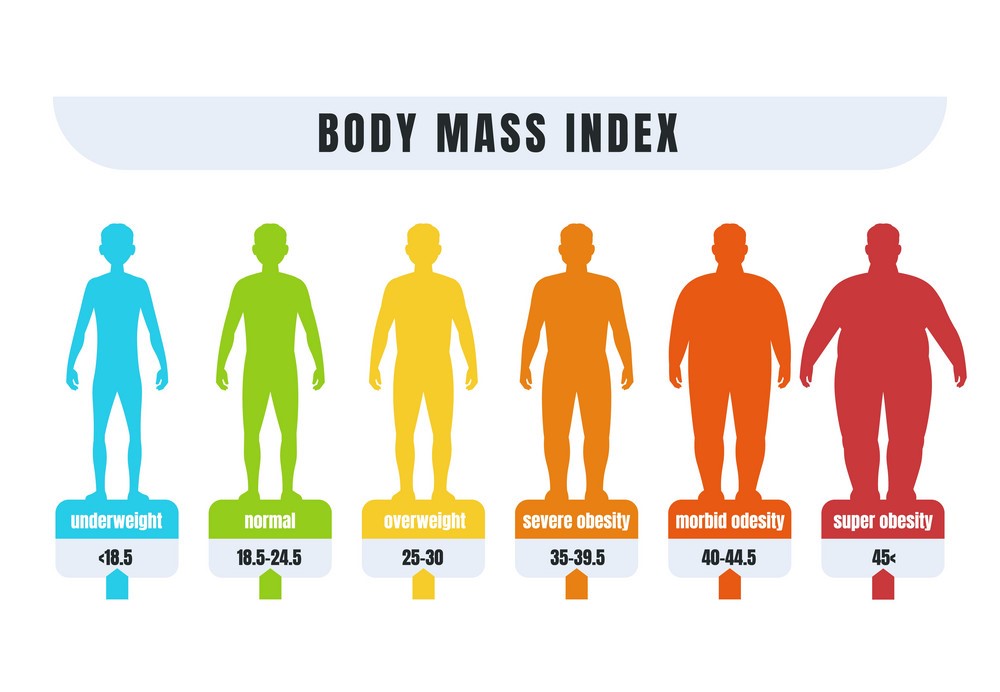
People are classified as overweight or obese based on their Body Mass Index. You can calculate BMI by dividing the weight in kilograms by the square of the height in meters.
A normal BMI range between 20 and 25, so people are obese when BMI exceeds 30 and severely obese or morbidly obese when BMI exceeds 40. Subjects with a BMI between 25 and 30 are among the overweights.
One of the disadvantages of BMI is that the calculation is based entirely on body mass and height and does not consider body composition. For example, athletes that carry lots of muscle but little body fat may be erroneously classified as overweight based on their BMI alone. For this reason, methods have been developed to accurately estimate the degree of adiposity by determining the body fat level.
Another criticism against BMI is that it disregards body fat distribution linked to health risks, as discussed later.
Methods to Determine Body Fat Level

Several techniques are available to determine the amount of body fat more accurately, which has specific advantages and disadvantages. Some are incredibly exact yet require costly hardware (DEXA). Other methods are cheap and easy but may have a significant measurement error.
- Fat-fold or Skinfold Tests
This measures the skin’s thickness – including the underlying subcutaneous fat layer. It’s done at specific sites across the body using a simple device, the skinfold caliper: front thigh, upper back, waist, and upper arm (triceps). The measurement is based on the assumption of a strong correlation between the subcutaneous fat layer’s thickness and the total amount of body fat.
- Hydrodensitometry
(Also called underwater weighing) and air displacement plethysmography is two different techniques that measure the body’s volume. Partitioning the weight by body volume yields the thickness of the body.
Body density can compute percent body fat using particular equations that assume constant densities for fat mass (0.9) and lean body mass (1.1). To put it simply: a more obese individual has a low body density and will float in water, whereas a very lean individual has a high body density and will sink in water.
- Bioelectrical Impedance
It involves sending tiny electrical impulses through the body and measuring their return. Since lean tissue conducts electrical impulses more easily than fatty tissue, less resistance correlates with a leaner physique. The significant advantage of bioelectrical impedance monitors is they are affordable and easy to use; however, the disadvantage is that the method is not very accurate.
- Dual-energy X-ray Absorptiometry or DEXA
It uses x-rays to determine body composition. This method is accurate and yields other relevant information, including bone density. A significant disadvantage is that the process is costly, and exposure to X-rays carries a negligible health risk.
↓↓↓ Please Keep in Mind ↓↓↓
- Non-obese adult males have a body fat percentage between 10-20%. Whereas non-obese adult females carry around 20 to 30% of body fat.
- Morbidly obese individuals can have a body fat percentage exceeding 50%.
- Body fat percentage gradually increases as people age because fat replaces the muscles.
Health Risks of Obesity

Probably the principal nutritional problem in today’s society is obesity.
- So why do we consider obesity a problem?
- Why are we concerned about obesity?
The main reason is obesity is associated with an increased risk of dying; we call that mortality. There is a clear relationship between your BMI as a measure of obesity and the risk of dying. And this risk especially goes up beyond a BMI of 30.
Several conditions are associated with obesity. But the most important is diabetes, which increases your risk of developing type 2 diabetes.
Besides, cardiovascular disease risk is also elevated with obesity & many other diseases like sleep apnea, stroke, pancreatitis, and arthritis. In contrast to many people’s perception, the risk for breast and colon cancer significantly increase in people with obesity.
On the other hand, there is a lot of talk about healthy obesity. Are there people that are obese but are still healthy? This is unclear, but this can be a very small minority. There is always some, even minor metabolic disturbance in people that carry too much body weight.
The significant metabolic disturbances in people with obesity are collected into one particular syndrome called metabolic syndrome. It refers to a collection of symptoms that often co-occur in one individual. And the most common characteristic of metabolic syndrome is abdominal obesity, carrying excess body weight, especially around the abdomen.
Another criterion for metabolic syndrome is hypertension, high blood pressure, cholesterol, and high triglycerides often referred to as dyslipidemia.
Finally, when people are obese, their bodies become less sensitive to the effects of insulin, called insulin insensitivity or resistance. Often, this is a pre-stage for the future development of type 2 diabetes.
So, obesity is a big problem; many will suffer from it, concerning the medical community about the risk of various diseases connected with obesity. Moreover, the crucial problem we’ll encounter in the next couple of years is diabetes type 2, which is increasing significantly in many countries worldwide.
Causes of Obesity

Obesity and Energy Balance
The energy balance model dictates that a positive energy balance MUST cause any gain in total body fat. Total energy intake exceeds energy going out over a prolonged time.
Thus, obese people must have been in a state of positive energy balance for an extended period to get to their current form, implying that they must have overeaten relative to their energetic needs.
It does not necessarily mean that obese individuals overeat compared to non-obese individuals. Studies have shown a strong tendency among obese individuals to consciously or subconsciously under-report their food intake, leading to underestimating their actual energy intake.
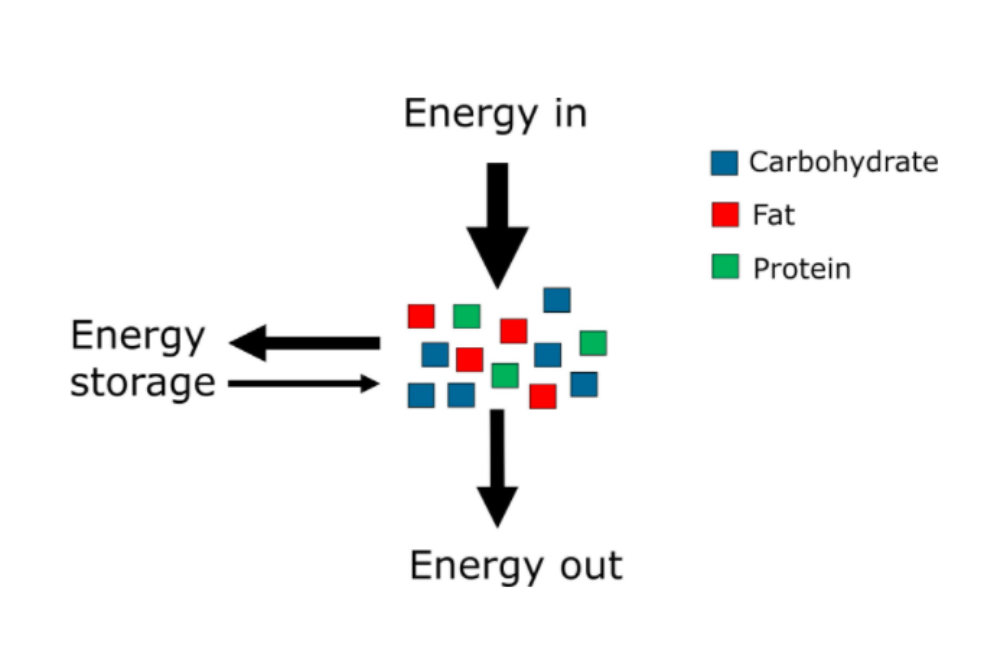
The positive energy balance leads to an energy surplus stored as fat, illustrating body fat’s critical role as an energy reserve. Although the body has ample protein stores, its size is much more stable and reacts minimally to energy balance changes.
WHY many people cannot maintain energy balance is a highly complex question that defies a simple answer. Obesity is the product of social, psychological, environmental, and genetic influences, forming the basis for behavioral changes that drive overeating.
Possible Solutions For Obesity
Dieting
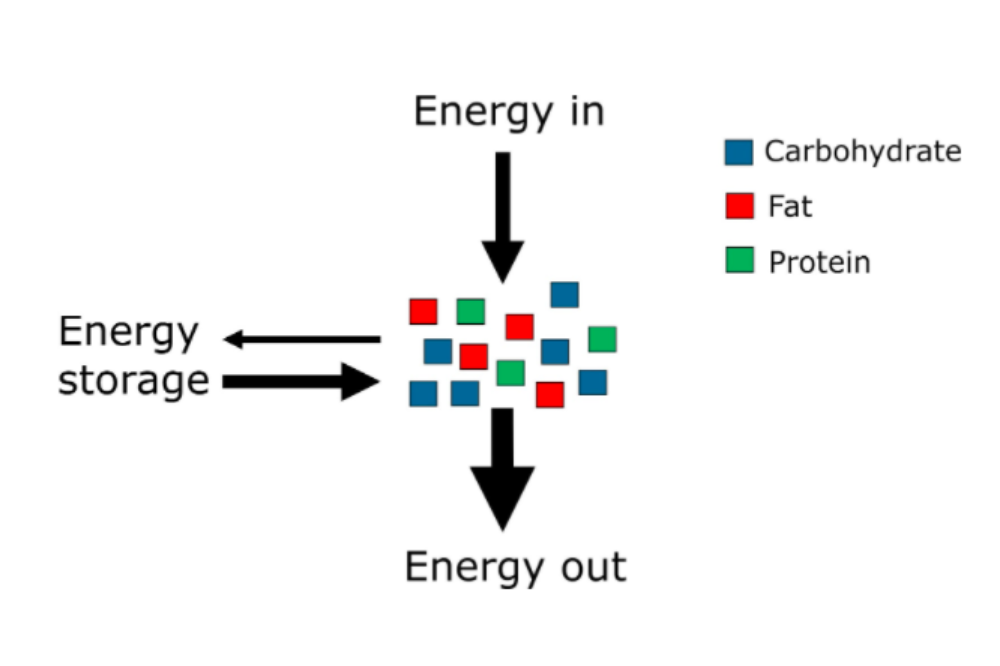
Weight loss requires a negative energy balance. The energy balance model dictates that a negative energy balance MUST cause any loss in total body fat. Total energy consumption surpasses total energy intake over a drawn-out period. Accordingly, you can lose body fat by diminishing energy consumption or expanding energy use. This rule is known as the first law of thermodynamics.
This notion – although mostly correct – needs some nuance. One could lower energy UPTAKE into the body without altering energy INTAKE, such as taking Orlistat, an inhibitor of fat digestion, or making other dietary adjustments that lead to more energy loss via the feces.
One should also realize that the Atwater factors for carbohydrate, fat, and protein are averages and may differ depending on the macronutrient source. As indicated before, protein digestibility is higher for protein in eggs than in legumes and higher for protein in white flour than in whole wheat flour. Switching from egg protein to wheat protein while keeping energy intake constant may lead to less energy UPTAKE.
Practically speaking, the impact of these subtleties is nearly hidden. It all boils down to those people who want to lose weight and should find a way to reduce their energy intake or increase their energy expenditure.
Nothing fancy. And a notion that any weight-conscious individual is well aware of.
However, the apparent simplicity of the message belies the complex, multi-factorial character of obesity. It ignores the fact that obesity is the product of numerous social, psychological, and physiological influences.
As a public health message, telling obese people to eat less is akin to saying that heroin addicts should stop shooting heroin or telling a person with clinical depression to cheer up. It is not that simple.
Immensely few people enjoy being obese or choose to be obese. They all would rather be slim. But they often feel trapped in their situation and cannot enact the changes in their lifestyle and eating behaviors to turn the tide. That hasn’t prevented individuals from attempting and brings us to the topic of dieting.
Weight Loss Diets
All effective weight loss diets are hypocaloric, which means they contain fewer calories (and therefore less energy) than the combined foods usually consumed.
Claims that specific diets can cause weight loss without reducing caloric intake are deceiving. All hypocaloric diets will result in fat loss. You could lose weight on burgers and fries if you consume fewer calories than usual. The overall energy deficit determines the magnitude of the fat loss. The bigger the cut in energy intake and the longer you can sustain it, the more significant the total fat loss.
The other thing that all effective weight loss diets have in common is that they impose restrictions that vary between diets but must result in fewer calories ingested. Examples of dietary restrictions currently popular include consuming special diet shakes instead of full meals, avoiding starchy foods (such as rice, bread, pasta, and potatoes), and eating exclusively between 12:00 and 18:00.
Is there any evidence that foods consumed outside the 12:00 to 18:00 time window are stored more readily as body fat? Of course not! However, because people are only allowed to eat between 12:00 and 18:00, they automatically eat less food and thus ingest fewer calories.
Avoiding starchy foods can raise the same argument. By removing these food items from the diet, there are fewer food items left to choose from, and as a result, people end up with a lower overall energy intake.
An example of a beneficial weight loss diet is the meat diet, which allows unlimited meat consumption and nothing else. This diet is helpful because people struggle to meet their daily energy requirements by eating meat. They develop so-called sensory-specific satiety.
Sensory-specific satiety describes the declining satisfaction resulting from consuming one type of food. Monotonous diets, therefore, tend to be highly effective in causing short-term weight loss. Simultaneously, because these diets are so dull, people have a tough time sticking to them and quickly return to their old food habits.
People have been incredibly inventive in designing new weight-loss diets, as attested by thousands of diet strategies proposed over the past few decades. Just visit the local bookstore to get an impression of the vast number of diet and weight loss books available to the consumer. The picture above presents a small selection of diet books. The scrutiny of scientific literature can draw several general conclusions.
- The more significant the overall reduction in energy intake, the higher the fat loss will be. And the most effective way to lose weight is not to eat anything at all.
- A significant restriction in food choice will automatically lead to a pronounced reduction in energy intake because of sensory-specific satiety.
- Dieting and concomitant weight loss inevitably cause increased appetite and hunger, the biggest impediment to staying on a diet.
- A high protein consumption elevates satiety and seems, by all accounts, to be the best system to stifle hunger sensations.
- The total fat loss determines the improvements in health parameters (i.e., reduction in blood pressure, triglycerides, and glucose) after weight loss. The current understanding does not depend on how the body loses fat (for example, rapidly vs. slowly, low-carb diet vs. low-fat diet, etc.).
- Small changes in caloric intake are not more effective at creating significant, long-term weight changes.
- Unfortunately, most diets fail, and people regain the lost weight (and some more). The long-term success rate of weight-loss diets is estimated to be below 10%.
Dietary Fat and Weight Management
Reducing fat intake has been effective weight maintenance and loss strategy for many years. The emphasis on dietary fat reduction peaked in the late 1980s and the 1990s.
An essential reason for targeting fat intake to achieve weight loss is the high caloric density of foods rich in fat. One gram of fat contains 9 Kcal compared to 4 Kcal for protein and carbohydrates.
Besides, saturated fat intake should reduce to lower CHD risk. The assumption was that singling out saturated fat would complicate the message. If people just reduced the fat content of their diet, they would automatically minimize saturated fat intake.
At that time, fat portrays as an evil substance based on most diseases of affluence. In response, food manufacturers tried to remove fat from their foods and serve them with low-fat labels, even containing very little fat.
Fat substitutes such as Olestra replace all or some of the fat in food and give it the taste, texture, and mouthfeel. Purchasers stayed away from high-fat nourishments for their low-fat variations.
Unfortunately, the low-fat craze did little to slow down the obesity epidemic that was gradually unfolding in many countries, including Europe and the USA. People disregarded the importance of calories and the need to achieve energy balance to maintain stable body weight.
Consumers shunned ice cream to prefer low-fat frozen yogurt, not realizing that frozen yogurt is still full of calories because of its high sugar content. Carbohydrates were viewed as excessive because the whole issue spun around dietary fat.
The women’s and health magazines led people to believe that all you need to do to lose weight is reduce fat intake, and you could consume fat-free foods in almost unlimited amounts. The overemphasis on reducing fat caused sugar consumption in our diets to soar. The low-fat hype’s failure illustrates the complexity of communicating with the public and putting out useful public health messages. As collateral damage, nutritional sciences’ credibility received a significant blow and will take years to repair.
One of the dangers is that consumers take a 180-degree turn and put the entire blame for the obesity epidemic on carbohydrates, as is happening today, and start to indulge in high-fat foods.
Nutrition scientists cannot emphasize the importance of total caloric intake, regardless of whether the calories come from carbohydrates or fat. They think weight control strategies should not be limited to a single nutrient.
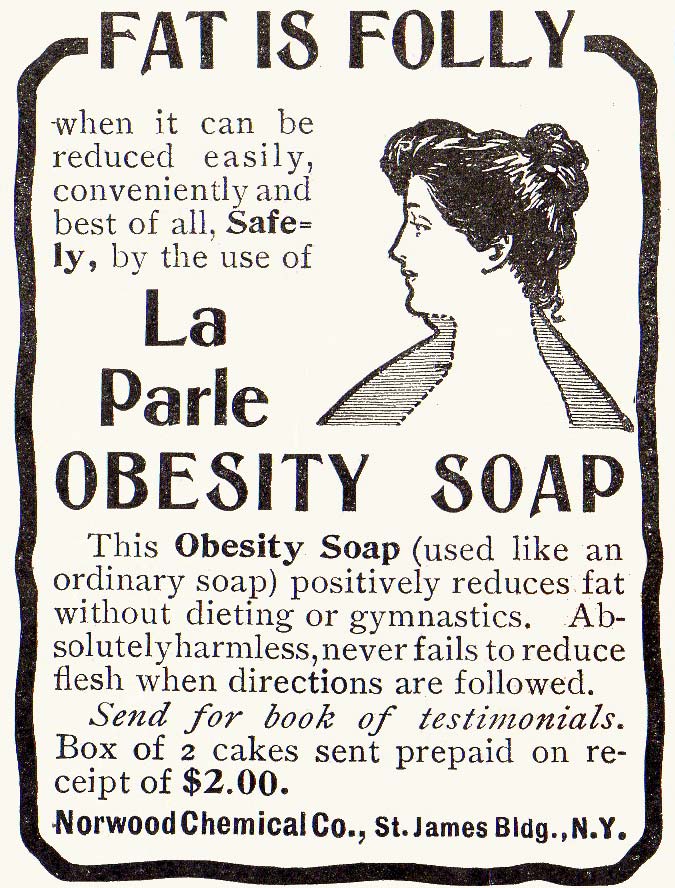
Increase Self-Awareness About the Weight Loss Products


Because many obese individuals are desperate to reach a standard body size, they are easy prey for the weight loss industry. The weight-loss industry’s annual revenue, including diet books, products, drugs, and weight-loss surgeries, has been estimated at 20 billion dollars in the US alone.
- The proverbial miracle pill claimed to burn fat fast, allowing you to lose weight effortlessly, does not exist.
- The herbal tea that helps people get rid of their belly fat is hype and a massive waste of money.
- The idea that lemon juice or raspberry ketones accelerate metabolism and encourage you to get more fit is absolute gibberish.
- And what about that sauna belt you put around your waist that claims to slim down your abdominal fat?!
You probably know the answer already. Human inventiveness and creativity seem to have no boundaries for concocting questionable new fat diets and weight loss products. Always remain highly critical concerning weight reduction items. If it sounds unrealistic, it undoubtedly is.
Featured Image Source: Pexels
I’m very happy to discover this website. I want to thank you for the time you spent giving your readers a fantastic read!!
I definitely liked every little bit of it and have you bookmarked to check out new things.